Left
hip. (there are some scratches on the film, left of center)
Left
hip. (there are some scratches on the film, left of center)In October 1996 I saw an internal medicine specialist for a bad case of poison oak. He recommended and administered a single dose of corticosteroid injected into my left gluteus. Five months later, on March 29, 1997 I felt a small pain in my left hip while cycling on a training ride. Within 2 days it was hurting enough to go to the doctor. Within 2 weeks, the pain so so severe that I was on crutches. An orthopedic surgeon in Santa Cruz guessed I might have early OA (osteoarthritis) but thought I had many years left before my cartilage would wear away. Further MRI and X-rays changed the diagnosis to early avascular necrosis (AVN, or "osteonecrosis") of the left femoral head. My symptoms did not match classic osteoarthritis. And, given the known association of corticosteroids and AVN of the femoral head - something my doctor did not warn me about - my confidence in the competence of the doctors I'd seen was shaken. My research in astronomy took a back seat as I began to spend weekends in San Francisco, at the UCSF Medical Library. Each week, I'd use my access through UC Santa Cruz to the on-line archives of medical literature, to read abstracts for everything related to bone, cartilage, and eventually on hip surgery as well. Then flag the most important papers and drive up to UCSF to read and photocopy the full articles before driving home Sunday night. I consulted a rheumatologist and asked him to give me a prescription for salmon calcitonin, (Miacalcin) which he did with reservations and only if I signed a long waiver beforehand. I contacted Orthologic Corporation and secured a donation of an Orthologic 1000 bone growth stimulation unit. Good research shows that applied oscillating magnetic fields will stimulate bone growth. I got Orthologic interested in researching their effectiveness in halting the progression of osteonecrosis. I used this faithfully for 6 months, into 1998. They showed continued interested in getting data on the utility of this device for AVN and bone cysts, after having success with it in healing non-union fractures. However in 1998 the unit was in need of re-initializing - and this could only be done by a doctor contacting Orthologic first. My doctors refused to do this, as new X-rays were not showing as strong an indication of AVN. It is quite possible that the bone stimulation unit and calcitonin saved my femoral head from collapse, and it is difficult to understand why I was not allowed to continue use of this treatment, given its complete safety and possible evidence of success in my case. In 1999 I contacted Orthologic again and was able to secure their agreement to send me their new unit, the Orthologic 2000. Like the previous unit, it could only be used for 6-9 months before the batteries needed replacing and also re-initializing to continue treatment (which approval was again denied). As further support of the steroid-induced AVN hypothesis, my right hip showed, and continues to show, no damage whatsoever. There is no history of osteoarthristis in my family, nor in my other joints. The 6 month lag between corticosteroid exposure and symptom onset is typical of this mechanism and also in agreement with the time scale for significant change in bone. By September 1997 - 5 months from symptom onset - all the cartilage in my left hip was gone. MRI's showed large fluid areas in the capitus area of the femoral head, and X-rays showed significantly diminished bone density in these areas. I was in severe pain for 3 years after this, requiring crutches to get around, 24/7.
After saving the femoral bone, my goal became to see if I could encourage regrowth of articular cartilage. After studying the works of Salter et al (1, 2, 3 and others, and here is a more recent paper.) I sought a prescription from a doctor for a continuous passive motion (CPM) machine. They refused, offering no reason, so I designed and built one myself, and used it for 8 months in 1998 and 1999. I have taken 1.5-3g glucosamine sulfate daily most days before and during the course of my hip disease, as well as a tablespoon of cod liver oil. I also began taking bone meal in 2001. By summer 2001 my hip began to feel a bit better, permitting periods without crutches.
Still, discourged by slow progress and influenced by a top surgeon (Lawrence Dorr) I asked to be scheduled for a standard total hip replacement in June 2000 in Los Angeles, CA. I examined the final X-rays taken the day before surgery, and I concluded that, contrary to Dr. Dorr's initial (early 2000) diagnosis of early AVN, they did not at this time show the classic signs of AVN which should have been advanced enough to be clear by this late date, 3 years after onset. Instead the X-rays showed large bone cysts. Dr. Dorr then looked, and agreed, but said I still needed hip replacement. I decided to cancel my surgery (a good thing, as these THR's turned out to be contaminated by machine oil! Patients who had these implanted had to have them removed, and thus lost ~10-15 years of life on their hip. Quite a tragedy). After much further literature study at UCSF Medical Library I decided to try intra-articular growth hormone therapy before any further consideration of hip replacement surgery. From Sept 2000 through January 2002 I submitted to intra-articular injections of recombinant human growth hormone (rHGH) by a noted surgeon in Florida. I did not see the success he claimed for his knee and ankle patients, and after reading about the short residence time of rHGH in the joint capsule and considering the different geometry of the (closed) hip vs the (open) knee and ankle joints he was claiming higher success with, I thought it worth one more try. I asked for a concentrated series of 3 shots within one week, and using a traction device I designed and built and took with me to Florida in order to separate the hip joint enough for the needle to access the joint space directly rather than simply the joint capsule. After 6 months of waiting for healing and not seeing the progress claimed for knee/ankle patients, I gave up on rHGH injections.
By summer 2001 my hip began to feel a bit better, permitting periods without crutches. By late summer 2002 I increased my dosage of calcium, settling on bone meal as the most promising form. I also increased my GS supplementation to 3 g/ day, based on a recent paper showing dose-dependent effects. My pain level decreased as my X-ray's began to show improvement in bone health - increased density, especially at the cyst sites. By mid 2002 I used them not at all. I have remained off crutches and my ability to do exercise has improved significantly. I'm now able to mountain bike up steep trails for several hour periods, swim with little pain, and walk (with a significant Trendelenburg gait) for up to a mile, and sleep relatively soundly. However, I have seen no further healing in my hip after ~early 2003. I am now of the opinion that while my bone quality is significantly improved, the bone surface is too damaged to hope for growth of articular cartilage. I believe the GS and cod liver oil have helped me maintain a thin coating of fibrocartilage - consistent with my symptoms and with a small but perhaps non-zero joint space on Xrays - and this with the bone partial healing has reduced my pain to a tolerable level.
I have been an active person all my life, competing in triathlons regularly until my hip degeneration. I'm 5'8", 142lb, and otherwise healthy.
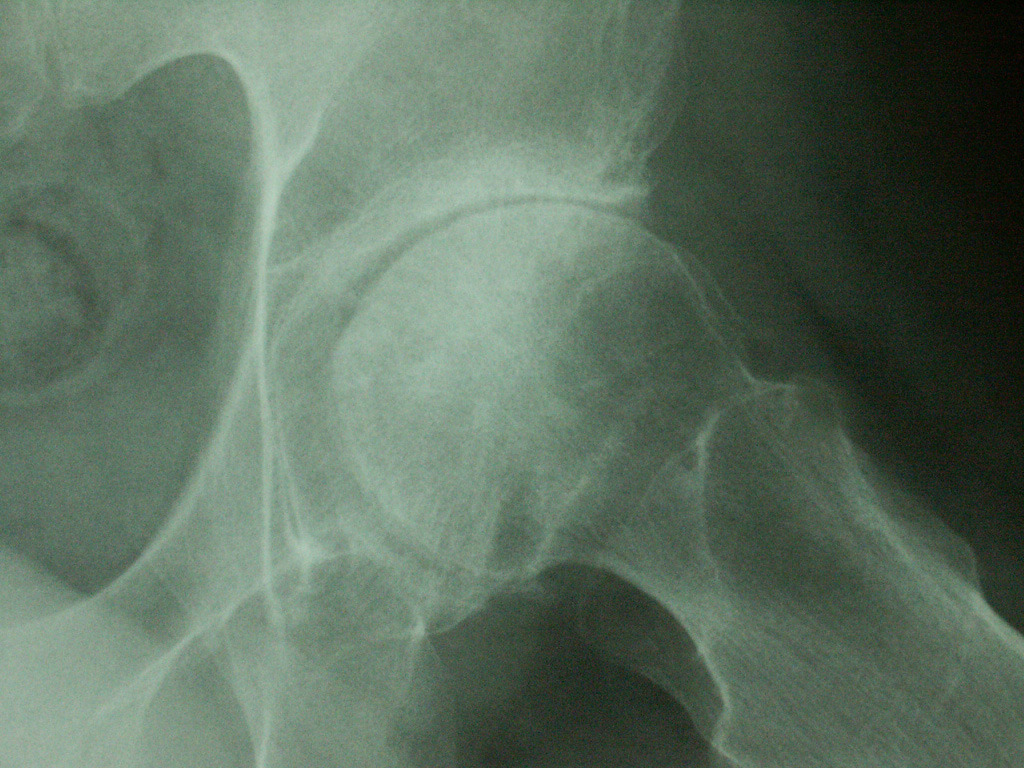
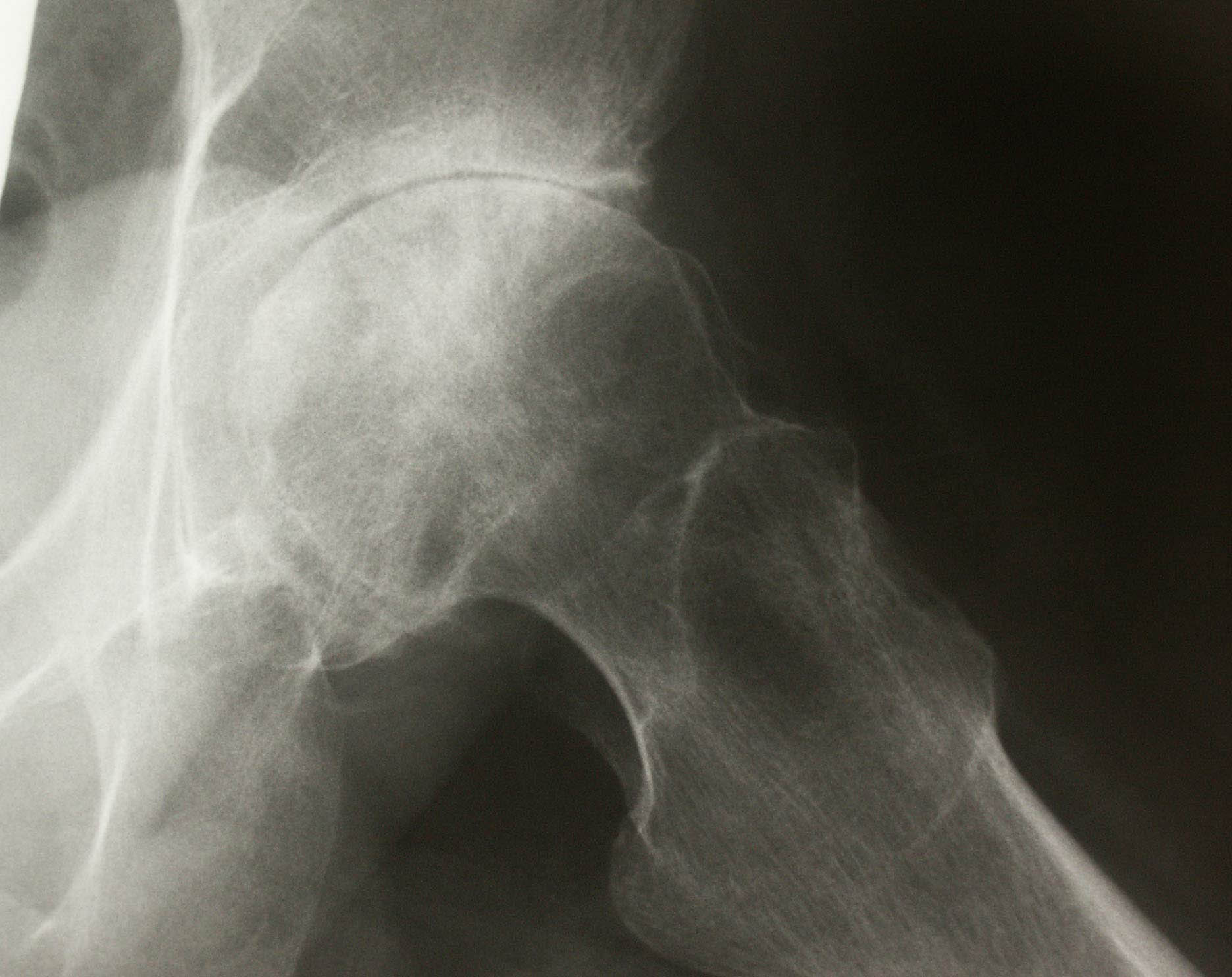
Some of my X-ray films are shown below. Click on the thumbnails to see a full screen high resolution view. I consciously tensed my muscles before each exposure in order to approximate the joint surfaces. In this way, joint space would have a better chance of indicating cartilage rather than simply joint fluid.
Large bone cysts are evident near the weight bearing surfaces of the femoral head. Bone spurring is minimal. There is a slight flattening of the femoral head in the weight bearing area, likely due to the corticosteroid-induced bone softening.
Left
hip. (there are some scratches on the film, left of center)
 Right
hip (normal, and remains so to this day)
Right
hip (normal, and remains so to this day)
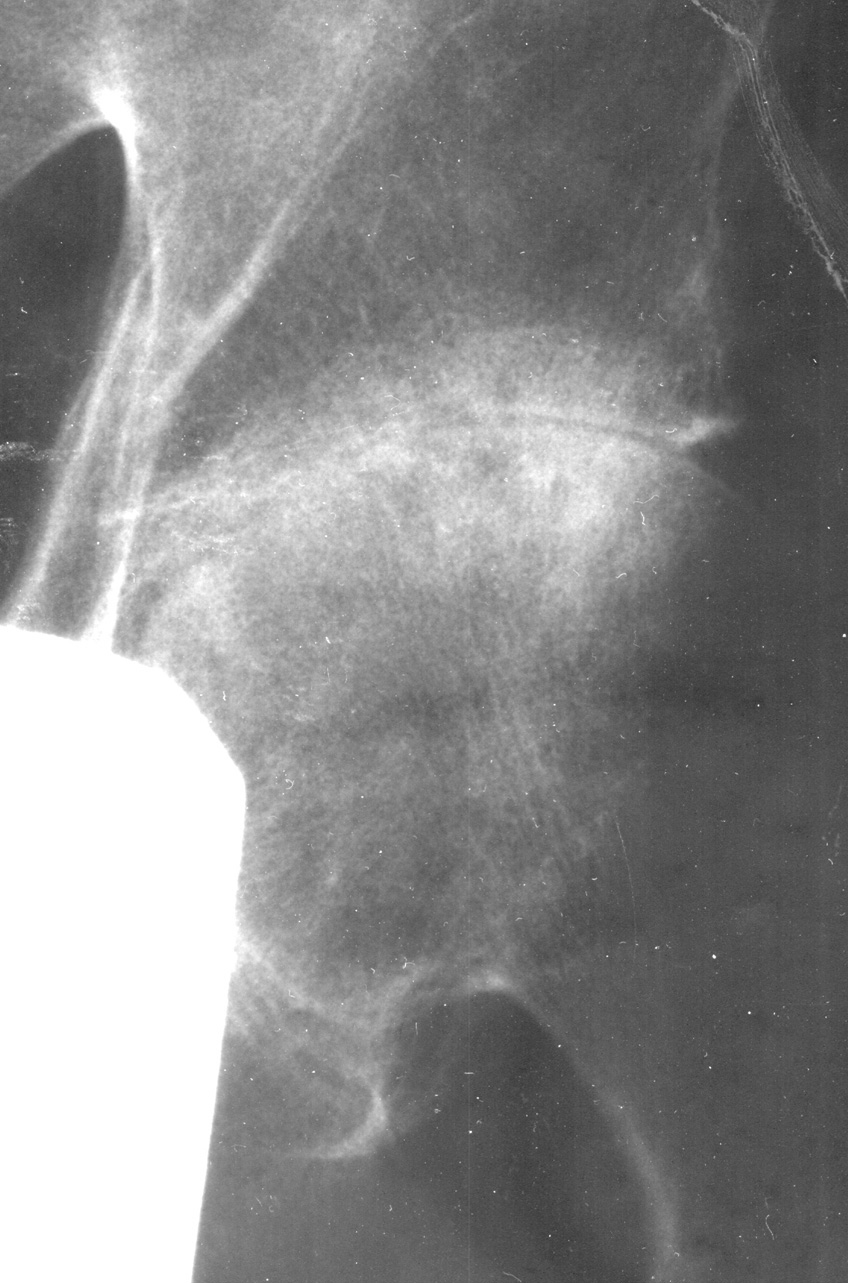
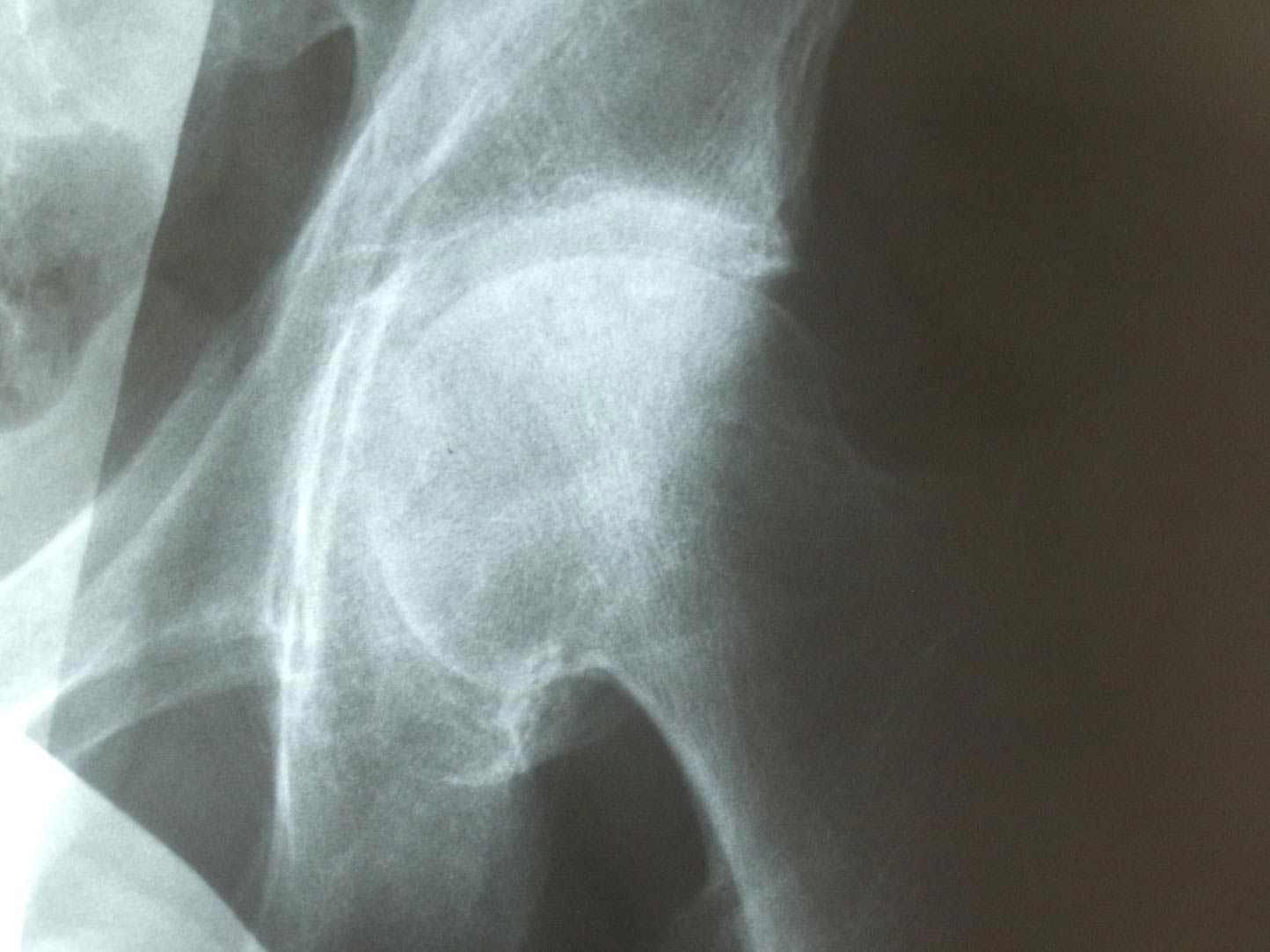
There is signficant healing of the bone cysts. Areas of low bone density in '99 and prior are now closer to normal here, although some sclerotic bone may contribute to this appearance. The slight flattening in the weight bearing area remains but has not worsened. There is no evidence of cartilage regrowth via joint space increase. The joint space shown in the "frog lateral" views is hard to judge, but the weight bearing surfaces shown in the first views show only 1-2mm of space, which is consistent with earlier views.
 Left hip.
Left hip.  Left hip - frog lateral
Left hip - frog lateral
The bone seems to show significant further healing. Bone cysts are now mostly healed. Trabeculation is visible in the subchondral areas of the femoral head which were not visible in 1999. There is sclerotic bone in places near the bearing points of the acetabulum and femoral surface, but these do not appear to have worsened with time.
 |
|
frog lateral view |
There are bone spurs which limit my motion today. These limitations were not as evident in the first 2 years, but became more so in early 2002, and have remained so but are not getting noticeably worse. I have little internal or external rotation in the left hip. Flexion is also affected, but I can flex to within about 35 degrees of thigh-against-chest.
I continue to get around without crutches. No further improvement in pain symptoms during this latest period. These latest X-rays are a bit overexposed and not as sharply focused, so with my Photoshop processing to get optimum contrast, it's harder to interpret the density variations in the femoral head. As with all films, I held my feet so that the toes came together and tensed my hip muscles to approximate the femur and acetabulum. Standard for hip X-rays. Possible increase in bone cysts and sclerotic bone in the capitus area. In late '03 I ran out of cod liver oil and did not get more until learning about evidence that fish oils inhibit the degradation of cartilage, and I began taking a tablespoon a day again beginning March 1, '04. For much of February, I felt an increase in hip pain; sharp pain similar to that in '98-'00. By March 14, my pain had again subsided. I interpret this as having worn through a thin fibrocartilage layer by Feb '04, and having regrown a bit after resuming fish oil supplements in March.
Since March '04 I've faithfully held to my schedule of 4 x 500mg capsules of glucosamine sulfate per day, a tablespoon of emulsified Norwegian cod liver oil, 800-1000mg calcium supplements as well as non-fat yogurt and plenty of green leafy vegetables for further calcium. Except for a few periods in '97-98, I have taken no NSAIDs or other pain killers beyond the natural remedies above (don't want to kill my liver and the rest of my bone/cartilage too). My pain level has remained the same; sometimes more severe for a day or 3 if I've had to lug around our observatory's large telescope in/out of my SUV, or excessive walking. With minimal walking, my pain level is uncomfortable but well beneath my threshold. I will get new Xrays soon, but have no reason from my symptoms to believe that they will look different than those taken last year below.
A standard "total hip" replacement (THR) is a bad solution, especially for someone still in their 40's or 50's as I am. They wear out, and particulate wear induces lysis of the bone and inflammation which leads to separation of the bone from the prosthesis. I didn't want a quick fix of a standard THR, only to look forward to most of my later years perhaps in a wheel chair, or severely restricted. After the failure of the rHGH injections, my hope instead was with a new surgery - surface replacement or "resurfacing", whereby they machine the femoral head to accept a metal cap, mated with a metal cup in the acetabulum. This solution gives normal hip geometry and no risk of dislocation, vastly reduced particulate wear debris and lysis risk, and a proven long term track record in Europe (which doesn't suffer from an FDA as we do). However, although I had maintained the most expensive medical insurance option Cabrillo College has, Blue Cross was denying coverage for resurfacings, claiming they were experimental. Only after FDA approval of the device I wanted would they cover. Unfortunately, this issue presented itself in 2001-2003, when my savings were wiped out by the stock market crash. I have no inheritance, no family help... and without insurance I couldn't afford the surgery. My dilemma was - wreck my financial future by paying out-of-pocket for a resurfacing, or wreck my future physical health by getting an inferior THR (which insurance would cover). Or... wait till the FDA approved the BHR device, the earliest and most successful of the resurfacing devices, and the only one in the late stages of the FDA approval process ("late" according to the opinions of those also waiting, and being in phase III trials). But would approval happen in a few months? That was the hope, although it might take as long as a year. The medical case for resurfacing is so strong that there was little worry of a denial of FDA approval - at least to my rational mind. So I waited... and in the mean time I also trained myself in the financial markets and became a much more active trader (trading, given my booked losses, now being a tax-free source of income if I could just learn to trade profitably. Compare that to having close to half my salary sucked away by the IRS, Calif FTB, the Cabrillo Union, Medicare, STRS,.....).
It wasn't until summer '06 that the BHR was finally approved by the FDA. By then, my homework had led me instead to the uncemented resurfacing device designed by surgeon Thomas Gross in South Carolina. Here is a parallel web page I put together which includes my first go'round with Dr. Gross and a surgery date in June '05.
I pick up the current story of my surgery with Dr. Gross below, after my X-ray history below...
As with all thumbnails, click on the picture to see a magnified detailed view.
The dark horizontal band is an artifact.The femoral head is still slightly flattened, but no more so than in the earlier series. |
Superimposing these with X-rays from '97 show no migration of the acetabular cup. This was determined by measuring the distance between the acetabular margin and the hip girdle arch at upper right, although in this projection this arch is perhaps not a completely reproducable marker. Possible increase in bone cysts and sclerotic bone in the weight bearing area. |
Frog lateral presentation. It's interesting that in the frog lateral views the flattening of the femoral head is much harder to see. This suggests it is very localized to the weight bearing point, which is rotated away from the image plane in these views. |
My normal right hip. The joint space shows no change from previous films, and the hip remains free of pain.
|
Bad left hip: The dark horizontal band is an artifact.The femoral head is still slightly flattened, but no more so than in the earlier series. |
Superimposing with X-rays from disease onset in '97 show no migration of the acetabular cup. This I determined by measuring the distance between the acetabular margin and the hip girdle arch at upper right, although in this projection this arch is perhaps not a completely reproducable marker. Possible increase in bone cysts and sclerotic bone in the weight bearing area. |
Frog lateral presentation. It's interesting that in the frog lateral views the flattening of the femoral head is much harder to see. This suggests it is very localized to the weight bearing point, which is rotated away from the image plane in these views. |
Dr. Koehn De Smet in Belguim studied this web page late in 2004 and said I'd have no problem as a candidate for surface replacement at his clinic in Ghent. He is a good option for those without insurance coverage. He's experienced, has good success, and is much cheaper than an out-of-pocket payment to any U.S. surgeon. So far, he exclusively uses the cemented BHR device. Since then, other overseas options for hip resurfacing have become available. Dr. Bose in India is one in particular who seems to be getting good reviews from his patients and early success rate.
X-rays were taken once again at the Radiology Medical Group in Santa Cruz. The scanner did not work this time with the transmission lid and the reflectance lid gave very poor scans, so instead I used my Dimage 5 digital camera and photographed the films on a fairly clean light table in the photo lab at Cabrillo College. In Photoshop I adjusted the brightness upward +27 on all images. No adjustments to levels, contrast, etc. Then cropped, sized, and saved for the web as .jpg.
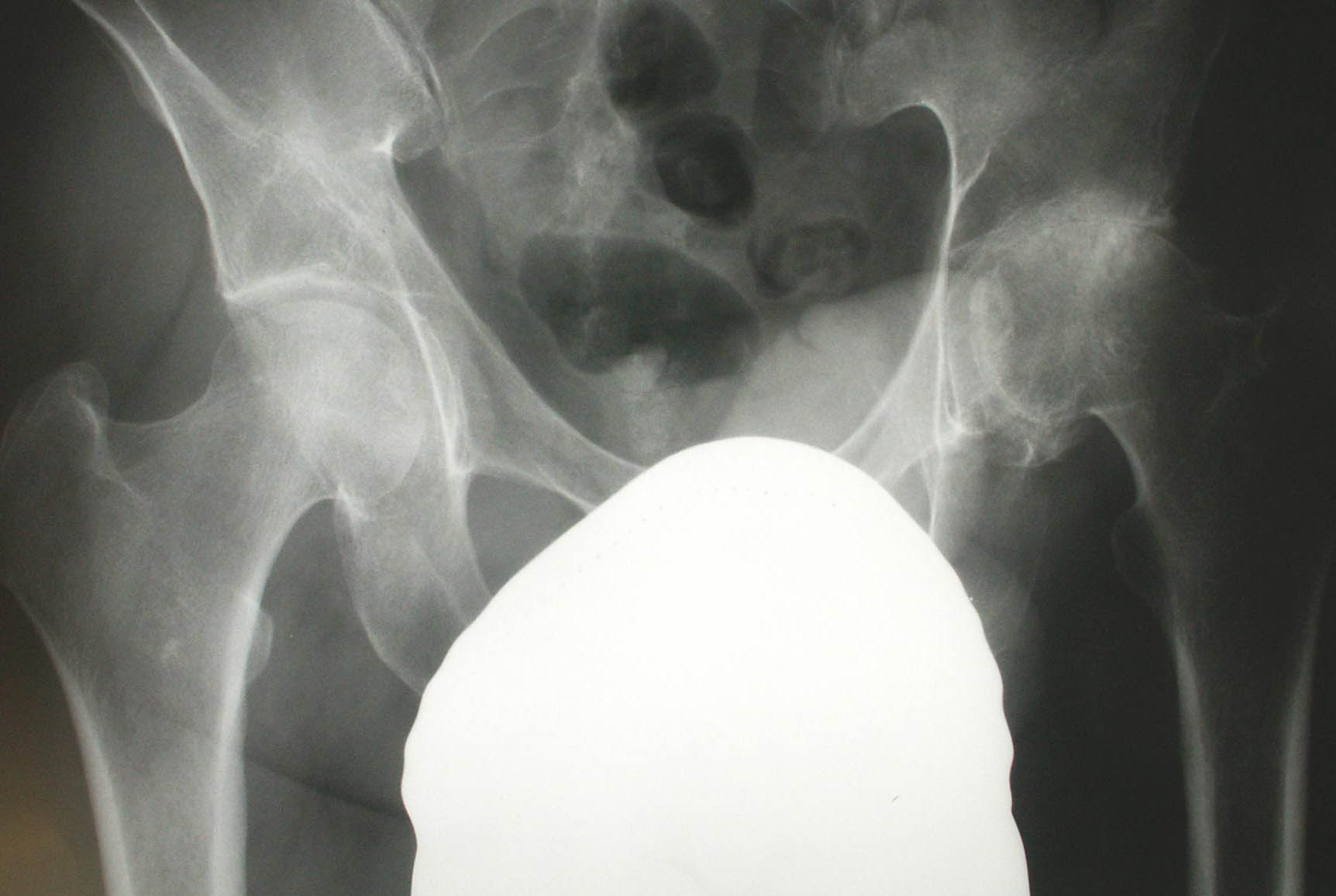
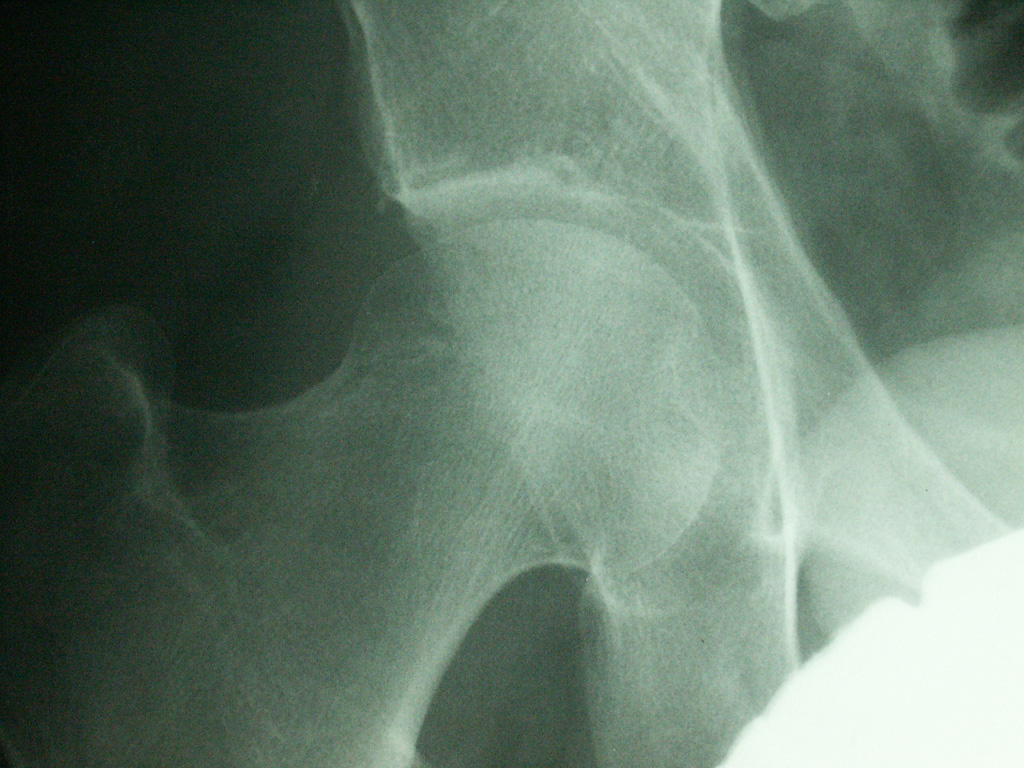
Symptoms have not changed during this past year. The right hip still shows no evidence of any degenerative changes. The bone density of the left hip area appears much less than on the right side; suprising since both sides have been used similarly; no cane or crutches this past year. |
The left hip alone. Trabeculation in the hip appears a bit stronger here than the films 1 year earlier. The density looks smoother throughout the femoral head compared to earlier Xrays. No further flattening of the femoral head is evident, although the weight-bearing surface might be a bit rougher. |
Frog lateral. The cresent on the right side of the femoral head is more obvious than in previous films; a projection effect with bone spurs, or something else? Not very evident on the view above which includes both hips. |
I was apparently not very symmetrically positioned on the X-ray table. However, I thought it still worthwhile to take the left side film and place it on top of the right side, aligning the outline of the femoral head and mid femur. I aligned using the inner of the concentric margins of the femoral head seen on the "left" film above. The flattening of the left side weight bearing portion is then seen to be very small, only about 1 mm. |
May 4, 2007
I have new X-rays as of last week. They show no change from the '04 Xrays despite the significant physical activity I've been doing, which I regard as evidence I've kept my bone fairly healthy (turns out, not so - keep reading...). The flattening is still there, and the joint space appears to be zero (but that's unreliable as an indicator, as geometry affects this 2-dimensional view). I'll scan and post them hopefully.
The prediction from Dr. Gross' office was that the Biomet cementless ReCap system would be available at the beginning of '06. Then, in Spring of '06. Then, in summer of '06. Then December '06, then.... There was clearly some hold-up, but despite my best efforts to pressure for clarity, I received none. Even letters to the President and CEO of Biomet. Then, as of early '07, Lee Webb at Dr. Gross' office was able to tell me that it turns out that they had unanticipated trouble in getting the titanium plasma coating to properly apply to the sintered beaded underside of the femoral cap. This was told to me, though, only after the issue was resolved. What else might be going on behind the scenes? Bill Deboer and I had some significant worries that it might be a business decision by Biomet, who looked about to be acquired by a larger company or by private equity, according to Wall Street research. Still, while this might mean a change in strategic initiatives, I could find no logical reason why Biomet might then decide to abandon this new design. It was clearly going to be a coup on their part and showed every promise of capturing a large part of the lucrative and growing hip replacement market. With increasing frustration, my best judgement still told me to wait till the cementless device was available. It was now nearly 2 years since I'd cancelled my cemented surgery. If I'd known it would be another 2 year wait, would I have waited? Tough to say in hindsight. But with the availability always relayed to me by Dr. Gross' office as "probably 4 months" away during this time, it was a case of Econ 101 in action. "economic participants always make their decisions on the margin". So - do I wait 4 months for cementless, or do I go now for cemented? That question always had an easy answer: Wait. I resisted making the unwarranted leap that "cementless is therefore ALWAYS going to be 4 months away". Tough, too, because all of my friends and acquaintances had long concluded that there was some neurotic reason why I'd waited so long for my surgery. Actually, there never was a neurotic reason, just a rational conclusion and a resistance to simply pouring myself into the hands of this or that medical authority figure. I'm pretty independent in my thinking and decisions - always have been. Long experience has taught me that trust in the medical profession is too often the fast track to tragedy. That was what had gotten this whole nightmare going in the first place. Clearly, I was not going to know of availability until it actually happened.. Ten years is 120 months, and every one of those months I was studying the latest information on my situation and what could be done, and making a decision based on that, as I've detailed above. I certainly never intended to wait 10 years. I'm used to dealing with scientists in astronomy and physics, where we love to share what we know and competitive secrecy is just not a big issue. This American healthcare system environment is different, and hard for me to fully adjust to.
Finally, the first set of cementless devices arrived at Dr. Gross' office in March 2007. By this time, I'd already made a surgery appointment for the next available time slot in my own schedule, June 13, 2007, right after final exams and ahead of a full summer of recovery. I was assured that my size range would be ordered and available. Next problem was insurance. Dr. Gross has been very successful at getting insurance approval, but one of his patients at this time (March '07) took it upon himself to call his insurance company - Blue Shield of California (unfortunately my company too) and ask point-blank about resurfacing. You NEVER do this! Let the doctor handle all insurance unless things go badly wrong. He's got more experience, and a financial incentive to get approval, since reimbursement rates are much higher than out-of-pocket rates. Blue Shield was now on alert, and denied coverage for resurfacing, claiming it was experimental. Argh! I knew what that likely meant for me. Sure enough, now I , too, was denied coverage upon submission of the pre-cert. After some soulsearching, I decided that even if it meant crippling my financial future by paying for all of this out of my own pocket (my stock trading had substantially rebuilt my savings from where they were in '01-'03), it was still the right course of action (compared to e.g. going to India, or Belguim, for BHR devices for a much cheaper price). But first, I located some legal details on Blue Shield's policy which showed that they were violating their own guidelines if they did not cover this. We combined this with the most recent medical facts backing up this surgery for my case in particular, and submitted an appeal. I thought for sure that it would again be denied, and I'd have to make a final appeal to the California Insurance Commissioner. After all, that's what insurance companies do with their 24hr day - they look for ways to NOT pay claims. That's how they make their profits. And, every appeal by other hip replacement patients to Blue Shield had been denied, according to the records on Surfacehippy. But amazingly, Blue Shield studied my appeal and reversed their policy! Now, for the first time, they would cover resurfacings and not just the standard THR's. It made both financial and medical sense, but still I was impressed that they capitulated. Later, as I monitored Surfacehippy, I verified that other Blue Shield of Californina patients were now getting approval as well. I stepped up my program of maximizing my physical fitness with one-legged mountain biking into the local mountains, and hard swim workouts in the pool. I'd need good upper body fitness while on crutches, and a strong right leg. I got my pre-op tests... not entirely good. My blood glucose was low, and my free testosterone was also low. My bone density was extremely low, worst of all was the most vulnerable spot - the left femoral neck. I did some more homework. Vibration platforms, such as made by Soloflex promised a way of increasing my bone density. However, the units felt under-powered to me, and the time was short (bone remodelling takes of order 4-6 months, and my surgery was now only 3 months away), and I worried that my extremely low density put me at risk for damage. Dr. Gross looked at my X-rays and pronounced that I was still a candidate for cementless resurfacing, and I did not want to jeopardize this - I decided to wait till after surgery before starting vibration workouts. If someone is still a year or more away from surgery and their bone density is only osteopenic and not osteoporotic, I think it's an excellent idea. It fits with every bit of homework and experience I have so far - the value of what can be called the paleolithic prescription - that we MUST do what our bodies have evolved us to do if we want maximum health. We're designed to eat lots of fresh fruits and vegetables, and to run. Studies show that it is impact which teaches bone how to remodel and stimulates growth for maximum strength. And that it is very much dose-dependent. The more you run, the denser and stronger your bone (see journal articles here). We're not evolved to get around in cars. We're designed to spend a large part of each day on our shoe-less feet, working and pursuing food. Not possible with my bone, but vibration promises a much more concentrated and painless way to similar a results, and early evidence is that it indeed does help post-menapausal osteoporotic women gain bone strength and density.
I focused on good diet; 1200 mg/day of calcium and co-factors, mostly in the form of lots of yogurt. Milk (yogurt) is designed by nature for consumption by infants to build bone rapidly (turns out milk or yogurt alone is not that great. More on that later). It's not just calcium that's needed, it's magnesium, potassium, phosphorus, vitamin D... I'd been with a good diet for some time, but clearly my body had eliminated "unneeded" calcium in my bones despite my good blood pH and chemistry. Use it or lose it, and after 10 years, I'd lost it.
My Week in South Carolina
I took a red-eye flight and arrived in Columbia at 9am on Tuesday June 12. There, my internet compatriot Bill deBoer met me. He was getting his 6 week checkup after getting his own cementless surgery in late April. I was in good spirits and feeling confident and ready to finally do this. I was also enjoying the feeling of no longer (for now) having to play my own doctor, studying and mastering things which are not in my field because I can't trust the medical people I'd dealt with. My read of Dr. Gross is very positive - he's clearly very bright, very committed, very much engaged in being the best surgeon possible and in designing the best system possible. On the phone, and in person, he quickly gets excited and animated when I delve into the lists of questions I have for him - he's not defensive at all, and he really enjoys thinking out loud and having intelligent conversations. Strange, and sad, but this is NOT typical of the medical people I've dealt with. He seems to have a high regard for me as well, which is also good. However, I'm an astronomer, not a doctor, and so I always find it stressful to have to be my own doctor.
 Unfortunately,
this was called for one more time... during my pre-op appointment, Dr. Gross
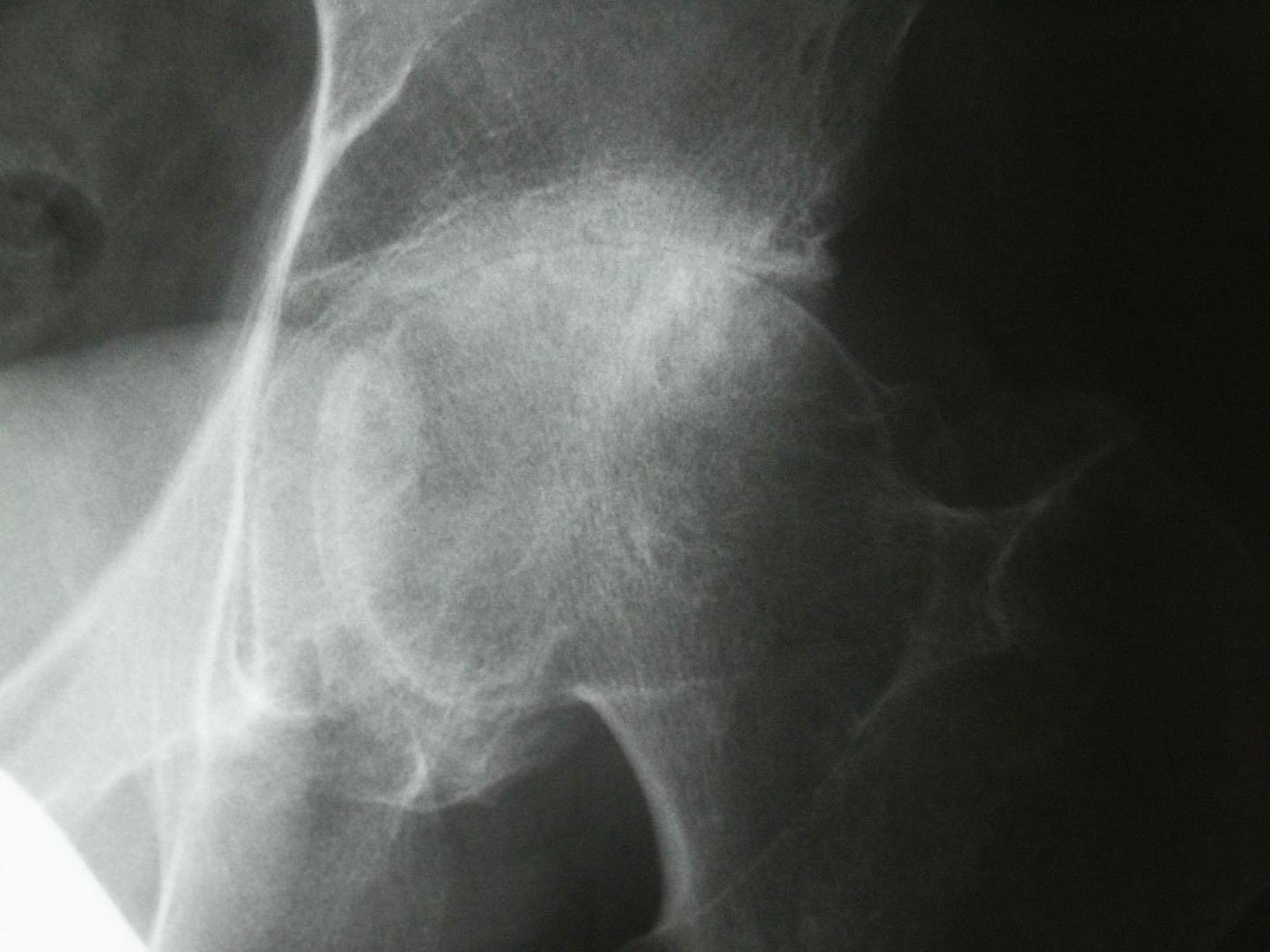
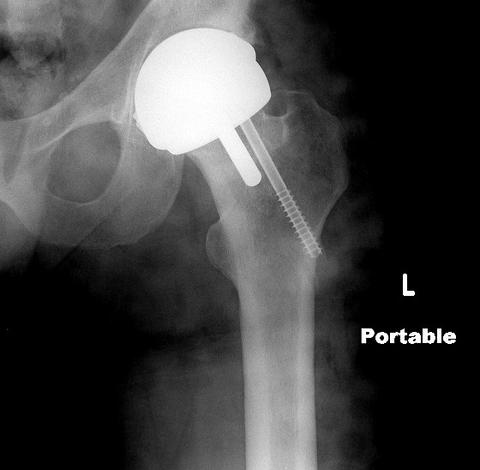
said he wanted to insert a titanium screw into my femoral neck. I'd already
seen another Dr. Gross patient who had had this done. He too had low bone density,
T-score of about -1.7 (his X-ray is at left). In fact, he was getting his checkup
at this same moment and so I could talk to him directly and see again the X-rays
of his hip. The screw has threads at one end, and has a taper at the other end.
Inserting it thus puts the femoral neck into compression on the top side. My
thought was that this would significantly affect the bone remodelling post-surgery.
The screw would be permanent. While I can see that it would provide some additional
strength against possible femoral neck cracking (still happens in about 1% of
patients, even if they follow the careful post-op guidelines - and Gross' goal
is to reduce this to 0%), the risk drops to near zero after 6 months anyway,
when the bone has strengthened. Did I want this screw in there for the rest
of my life, given that my intent was to return to regular running? I asked Dr.
Gross to "sell" me on this screw, but he would not, preferring to
leave it up to me whether I wanted it or not. Apparently, there are no studies
which support its use long term. It's just a common sense attempt to reduce
fracture risk. I spent the night before my surgery in the Courtyard Marriott
hotel across the street, visualizing this screw and seeing analytically where the stresses
during impact loading would go, factoring in the different compliance of the screw vs. the bone, and the fact that the anchoring was via a few screw threads into low-density
bone... I just could not make a good case for a permanent implant of this screw
into bone which had no fractures. Especially including the dangers of doing
the drilling of the bone in order to insert the screw in the first place. I
also had to face the possibility, however, of having a femoral neck fracture
later and having directly gone against the advice of my surgeon. I looked at
it all, carefully, for hours, and then got some sleep. I was not sure I'd be
seeing Dr. Gross before the anaesthetic took effect, so I wrote up a note and
pinned it to my shirt, explaining my choice - no screw please!
Unfortunately,
this was called for one more time... during my pre-op appointment, Dr. Gross
said he wanted to insert a titanium screw into my femoral neck. I'd already
seen another Dr. Gross patient who had had this done. He too had low bone density,
T-score of about -1.7 (his X-ray is at left). In fact, he was getting his checkup
at this same moment and so I could talk to him directly and see again the X-rays
of his hip. The screw has threads at one end, and has a taper at the other end.
Inserting it thus puts the femoral neck into compression on the top side. My
thought was that this would significantly affect the bone remodelling post-surgery.
The screw would be permanent. While I can see that it would provide some additional
strength against possible femoral neck cracking (still happens in about 1% of
patients, even if they follow the careful post-op guidelines - and Gross' goal
is to reduce this to 0%), the risk drops to near zero after 6 months anyway,
when the bone has strengthened. Did I want this screw in there for the rest
of my life, given that my intent was to return to regular running? I asked Dr.
Gross to "sell" me on this screw, but he would not, preferring to
leave it up to me whether I wanted it or not. Apparently, there are no studies
which support its use long term. It's just a common sense attempt to reduce
fracture risk. I spent the night before my surgery in the Courtyard Marriott
hotel across the street, visualizing this screw and seeing analytically where the stresses
during impact loading would go, factoring in the different compliance of the screw vs. the bone, and the fact that the anchoring was via a few screw threads into low-density
bone... I just could not make a good case for a permanent implant of this screw
into bone which had no fractures. Especially including the dangers of doing
the drilling of the bone in order to insert the screw in the first place. I
also had to face the possibility, however, of having a femoral neck fracture
later and having directly gone against the advice of my surgeon. I looked at
it all, carefully, for hours, and then got some sleep. I was not sure I'd be
seeing Dr. Gross before the anaesthetic took effect, so I wrote up a note and
pinned it to my shirt, explaining my choice - no screw please!
My Surgery
Things got off to a bad start. After my appointment with Dr. Gross, still the day before surgery, I went to Providence Hospital for a final blood draw for blood typing. The nurse there was not skilled, or not careful, or both. I didn't have a good feeling right away, and Edie (was her name) punched right through my vein and out the back side. It hurt. And within a half hour there was a large hematoma bulge under my elbow. I had mild shock reaction, but after Bill and I considered (we were having dinner across the street at the Cracker Barrel restaurant) going back to the hospital.... I decided to just tough it out. What could be done anyway? It stabilized, and I knew it would be ugly, but not catastrophic.
5:30am June 13, my alarm goes off. My blood-draw left arm is a purple mess. I dress, and take my crutches and hobble off in the pre-dawn skies to the hospital (Providence Hospital) down the street. I'd made a mental note to look for the cresent moon, which was making a spectacular occultation of the brightest star cluster in the sky - the Plieades - at this very moment.... but forgot. I waited in the lobby for a half hour, then a male nurse got me and took me back, where I got out of my clothes into a gown, packaged up my things into a locker, and laid on a gurney. I was given some pills. I was told to mark with a Sharpie the word "yes" on the hip to be operated on (sounds funny, but I think that's a great idea). The anesthesiologist came in and asked me about my glucose levels. I told him that my recent tests showed it was out of range on the low side: 57 and the normal range was 70-120. He was concerned somewhat, and wanted to review my blood work, which the hospital didn't seem to have immediately there. Fortunately, I had copies and carried them with me in my daypack. He also ordered that one more blood draw be done and get a new glucose figure. It's important, because if it's too low and there's too much anesthesia given, it's dangerous. He explained that I would not be given a general anesthetic - a "general" makes for a harder and more prolonged recovery. Instead I'd get a spinal anaesthetic and then a sedative. He said I wouldn't be getting regular morphine, I'd be getting AstroMorph (no joke!) - which certainly sounded like the good stuff to me. Still, I'd be "awake" more or less during this operation. If you look at a video of a hip replacement operation, they're quite violent. "OK", I said to myself - "others have done this, so can I". The blood draw was in the same arm (left) as the bad poke from yesterday, and this one did not go well either as I later found out. My right arm got an IV inserted also at this time. My left hip area was shaved and swabbed with betadine. The sedatives began to take effect and I drifted into a state where I could hear what was going on, and feel my body moved, but found it hard to feel much else.
Then, the drugs really took effect, and I had a pretty interesting experience. I knew who I was, I knew I was in Columbia, South Carolina and that at that moment my left hip was being opened up, but that awareness was eclipsed by the visual light show inside my mind. Vast desert landscapes passed below me at the speed of sound, with pastel reds and oranges morphing into mountains and canyons which eroded through speeded-up geologic time. I could hear voices, but couldn't quite tell what they were saying. I could feel my hip being worked on, but the pain was quite dull. I felt pressure there, and discomfort, but not enough to cause any physical recoil reaction. I knew from my homework what was happening, but I couldn't tell where in the process I was. Was he slicing my rotator muscles? Was he drilling into my trochanter for a measurement? Was that tug the dislocation of my hip joint? Was that my femur now protruding outside my skin? Was he hammering on the cap? I felt emotionally detached, and just watched the drug trip play out. It went on a very long time. I went under at about 7:30am. The voices began to get clearer now, and I strained to make out some word or phrase that would tell me whether I'd been sewn up yet. I heard the word "recovery room" and knew it must be over now. After a while, the desert light show gave way to the real world somewhat, and I opened my eyes and saw the time - 12:40pm. 5 hours. I thought, that's a long time. I wonder how much blood I lost? (turns out only 100ml - good work, Dr. Gross!) Did something go wrong? The surgery itself I thought would only take 2 hours at the most. No, nothing had gone wrong, just an extended dream time. But there were a couple of nurses now around me. Asking me.... something. My speech was glacially slow. I stayed "out of it" for a while longer, as they wheeled me out of the recovery room and into my private room which would be my home for the next 2 days. I was still quite groggy and unable to do much besides take in my surroundings.... and saw the TV on the wall was on. Something on CNN or maybe the weather channel, and major storms brewing in central South Carolina. Hmmm, that's right here, I thought. Big red blotch on the national map. Tornado watch they said. Great, I thought. When I could move my head, maybe 5-10 minutes later, I looked out the window and saw lightening strikes. More lightening, closer. And then, weird electrical sounds. And people running around. Turns out the lightening had hit, and my hospital bed (a high-tech thing) had fried. They struggled with it. I thought I should marshall my capacities and think what I should do... but I just couldn't. I had wraps around both legs which rhythmically pressured and de-pressured my calves in such a way as to prevent blood clotting. This unit too, had fried. At some point, they found another bed, wheeled it in, and moved me onto the new bed. I heard that the computer at the nurses central station which monitors patients vitals, had also been zapped by the lightening. I tried to think through what that would mean for me, but just couldn't make my mind work. I'd been looking forward to a time when I could just go with the flow and not have to think so decisively so much, and I hoped that that time had arrived... but being too drugged to deal with this new situation, isn't what I'd looked forward to. Up most of the night, as nurses came in and monitored, poked me with needles, fed pills... Didn't sleep much.
Dr Gross came in at 6am the next morning. I asked him what he thought about my bone quality, now that he'd actually worked with it under his own hands. "It's weak" he said. Another issue was a small area of non-contact around the circumference of the femoral neck, and 3 small bone cysts which needed to be grafted with his magic paste which he makes from my blood and bone chips from the acetabulum reaming. But he felt these were non-issues long term. He gave me an image of my new hip, and also gave me the surgical report (I'll see if I can scan this and link it here, sometime later).
For the next 2 days, I was poked for more blood, measured for blood pressure, temperature, oxygen saturation (always 96-100% - excellent) , and given a wide range of pills around the clock. I was also taught how to give myself shots of Lovenox (a blood thinner) into my stomach. I was to do this each day for the next 10 days. My hip was swollen, but not as swollen as I'd feared. I was given an ice machine - a "playmate" sized unit which had an aquarium pump with it and circulated icewater through a wrap covering my hip. Still, it hurt, more than I thought it would. I'd brought books, but was too headachey and pained to actually read. Mostly I watched TV or tried unsuccessfully to sleep. I was fed 3 meals a day, but given the state of current knowledge of nutrition, I was disappointed. I saw no fruit at all, the rare salad was iceberg lettuce, and mostly it was southern food - meatloaf, canned vege's, biscuits and gravy, corn grits, sausage, dry stick-in-the-throat white-flour pancakes. Where were the calcium supplements and vitamins I needed? I had brought some with me, but I wished I had more. I expected the calories would not be quite this empty. Every 2 hours someone came in for something... 10pm, midnight, 2am, 4am, 6am.... combined with the pain, I just never got any sleep. I calculate that I got a total of maybe 4 or 5 hours from Wednesday (surgery day) through Saturday when I checked out. It left me intensely tired and with a significant headache (I never get headaches!). Then there was the constipation. The drugs. My last BM was 2 days before surgery. Finally, on Saturday, I had some relief. On Thursday, a cute PT came in (Elizabeth) and helped me crutch my way up/down the hallways. I was taught the 3 exercises to do - toe pointers, leg lifts, and knee lifts. Pretty straightforward. They checked carefully the pulse and strength of my operated leg. Absolutely no nerve issues - felt just as good and strong in that regard as before surgery. My last night, at 4am, the dreaded "nurse Rachitt" showed up to do another blood draw. I showed her my left arm, by now a large purple and black swollen mess, and she said "I didn't do that". I said "yes, you did." She was in automated mode, pulling my arm and trying to poke me as quickly as possible. I recoiled, and begged her "PLEASE be careful!" She said "don't be pulling your arm away". PLEASE be careful this time! "We gots to do our labs". I extended my arm, and this time she was careful enough to get it done without the hematoma.
Getting Home - the Nightmare I Couldn't Wake Up From!...
The first of my three connection flights had a departure on Saturday, 2:10pm. I called the recommended taxi service and was ferried to the airport. I'd arrived in South Carolina with just a day pack, but now I was leaving with the day pack and also a new cane and a box which had my ice machine. My taxi driver helped me get the box checked at the airport. The cane and daypack stayed with me. I felt miserable - splitting headache and tired beyond words. I would not recommend that people get major surgery and then fly across the country with two connecting flights, alone, 3 days later. As I looked at the side-effects of the various drugs I'd been on, first on the list always was nausea. ...Perfect! I'd not really had trouble as long as I was essentially motionless in bed at the hospital, but I was worried about the plane flights, even though I never get airsick. First flight was on a tiny prop plane just over the border to Charlotte, VA. Weather didn't cooperate - storms, rain, lots of convective air motion for our little plane to get through. I kept my eyes closed tight and head in my hands and endured. I was sick to my stomach, but didn't hurl. I was not looking forward to my second flight (US Airways - which Bill said they refer to as "useless airways", and which I just found out had the worst on-time performance of any airline.). Just perfect, I thought. They were taking me to LAX for my final connection to San Jose. It was an awful flight. Keeping my leg at greater than 90 degrees (the first of 3 rules) while trying to cradle my head ... I kept my head in my hands and eyes closed and focused second by second on not throwing up. One second. Then the next. Then the next. In fact, before boarding, I went into the airport john and tried to empty my stomach but was unable to. Boy was I miserable! Miserable!! Finally, over Texas, I lost it. (Texas, I suppose, seemed to my system to be a good choice). Barf bags were used and the absolutely full airplane got to intimately experience my situation. No help in getting myself cleaned up, but a passenger did finally go back and get some wet towels for me. The flight attendants just looked at me pathetically. After an infinitely long flight, I arrived at LAX. Here's where things got worse. I got a wheel chair ride to a shuttle, but when the shuttle got to where it was going, he couldn't get me any help. Finally, almost out of time, I got my crutches and headed off in the general direction of the security area. Going up a floor, left. There it was - security for American Airlines. There, I was asked if I could go through security without my crutches. No way - I am forbidden to put more than 10% of my weight on my left leg for 6 weeks. I had to separate from my daypack. They took me out of line, sent me off to the pat-down area. Patting my left leg, I gritted my teeth. Meanwhile, my cane and day pack were making their own way through security somewhere else. Then they checked for shoe bombs. Very tough getting in/out of my left shoe. Finally, they turned me loose. I found my daypack, but my cane was.... gone. No time now to track it down, I crutched madly down the long terminal. Sign said my flight left from Gate 44I. 44I? Strange gate letter. At long painful last, I get to the end of the terminal, and see the gate numbers... 42, 43, 45, 46. What? No 44's. Was this terminal in the Twilight Zone?? Gah!! I try to get the attention of an American Airlines person, but he ignores me as he deals with someone else. Finally I find a floorsweeper and he tells me I have to go all the way down past the Chili's restaurant and then go down a flight of stairs and then take a right and then get to a road which... ?! I just look at him, but he assures me this is right. More mad crutching, and I find the Chili's and then the stairs and then the right turn and then exit and there I am right on the landing tarmac. I look around... can this be right?? I'm directed to a shuttle, which says that the gate 44's are for American Eagle and have their own building somewhere elsewhere. A mile of more travel, dodging airplanes as they taxi and take off right in front of us. OK, I arrive at the 44 terminal and find 44I at the very end. Now I'm really suffering, but I made it, and loading commences. Once again, I put my head in my hands and close my eyes and just focus on not barfing on this final airplane flight to San Jose. Stomach empty, I make it, and this time get a wheelchair ride down to the baggage claim area. I phone Karl and Carla tells me he's down there somewhere waiting for me. He finds me. We wait for my ice machine.... and wait. Finally, the baggage roundabout stops turning and everyone's gone home. The building is dead quiet. I wonder again - Twilight Zone?? The sign over the roundabout never does say "American 3131", but I'm assured that this is where it would be, and saw other passengers from my flight there too. Just perfect. They lost my luggage. I fill out forms, and load myself into Karl's Saturn for one more stomach adventure over Highway 17 and the Santa Cruz Mountains and arrive after 1am (Eastern time) at the Delucchi's. 12 hours from hospital to home, and I had counted every miserable second. Others who read this and are getting surgery - I don't recommend my experience. Find another way if you can. Short of a flaming plummet from the skies, it's hard to imagine a worse flight experience!
Three days later, after receiving loving care from all my friends, I'm now home and having gotten sleep finally, am feeling better. My ice machine even showed up at my door (eventually)! My cane... gone forever. But no biggy. I'm home and recovering!